Context
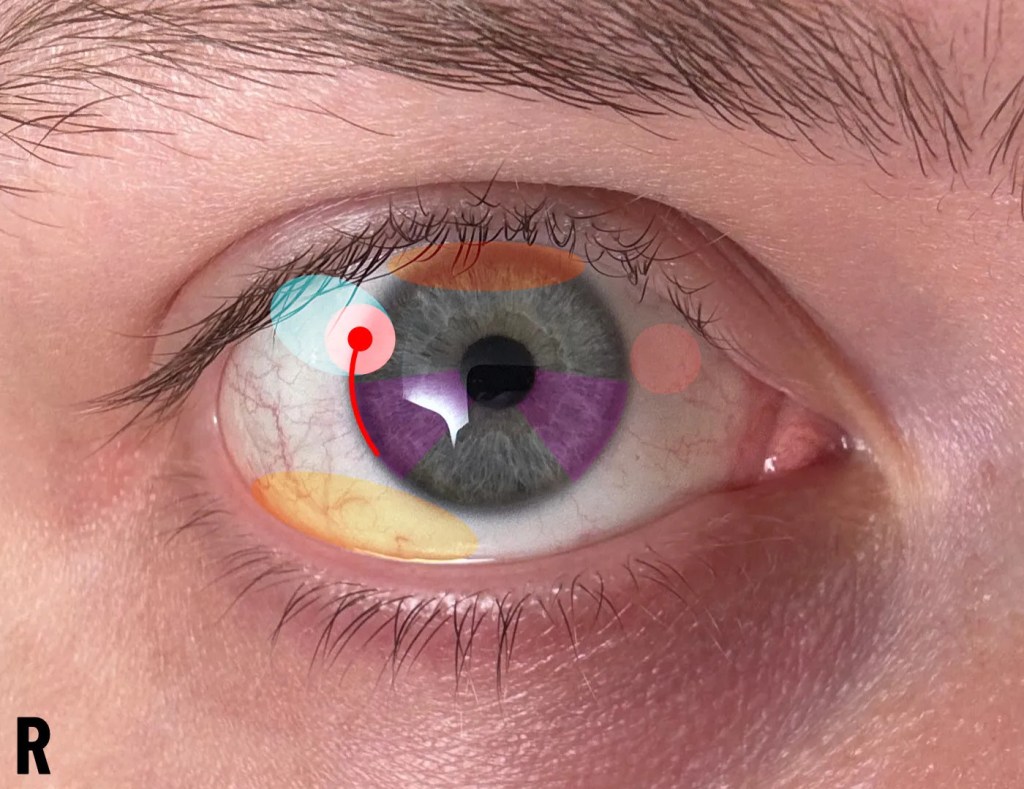
In 2024, I privately attended an eye hospital in London and was seen by two consultants. This was not the first attempt to get clarification on the issue, as previous advice had been sought from opticians who could not interpret the descriptions of symptoms and decided not to refer on the basis of not knowing. An example of such descriptions were ‘a spiking pain sensation that appears in two specific places in the right eye, along with a constant burning in the inner side of the eye, however this burning sensation disappears if the opposite eye becomes irritated’. These descriptions were perfectly sufficient for the final consultant who would later become a professor of corneal regeneration. The first phase of opticians did not consider referrals when an answer was not clear. A referral to an expert at a higher station would be the most appropriate course of action. It raises an issue of modesty in local, independent healthcare, such as opticians balancing independent interests alongside NHS MECS (Minor Eye Conditions Service/s). In this case, self-referral was required to pursue help at the London eye hospital.
Treatment Path
The first consultant was inadequate for identifying corneal neuralgia post-abrasion-recovery, whereas the second managed to appropriately identify and diagnose the issue, making reference to previous patients with similar presentations.
After the first failure, feedback was provided to the hospital, noting both the lack of specialist education for corneal neuralgia issues, along with the lack of in-vivo corneal confocal microscopy equipment sufficient for diagnosis. No response was received.
The first-line (and simplest) therapy provided was a continuous low dose of a ‘soft’ steroid to assist natural recovery, being hydrocortisone sodium phosphate (C21H29Na2O8P). Though not discussed, it is discoverable knowledge that autologous serum tears are a suitable topical therapy for nerve regeneration. Investigation was done into the viability of producing autologous serum tears from home in the case of sufficient skill and hygiene, and the lack of diagnosis and help. It is possible, but not recommended. The equipment is available to me now, however a management plan is in place for long-term management of persistent issues with the eye. This was made more complicated due to the local GP not adding the steroid to my repeat prescriptions despite my ophthalmologist repeatedly asking via report. I have resolved to stop asking and use another method to force them if needed.
Over the span of a few months, the profile of pain, stinging and burning sensations did reduce alongside steroid use, however reactivity of the eye to irritants did not reduce (and has still not, a couple of years on). This requires constant management via eye rinses under tap water, preferably soft water as it feels less abrasive than hard water. There have been no side effects of doing this for two years.
Regarding efficacy of the steroids, the theory is that an over-active immune system will respond to abrasive nerve injury by clustering immune cells and persistently releasing inflammatory cytokines and suppressing nerve regeneration, or forcing the nerves to regenerate in a way considered structurally incorrect. Steroids may reduce immune activity, thereby giving nerves a more suitable opportunity to regrow.
Note that thiamin supplements were occasionally taken alongside the steroid due to anecdotal reports of assistance with nerve growth. B12 was also taken continuously with vitamin D and folate. I cannot speak to the efficacy of this, but careful, non-excessive inclusion of such vitamins was decidedly quite harmless and worth a try.
The topical steroids eventually started causing gastric issues and a probable gastric ulcer, leading to the cessation of steroid use until a gastroenterologist could investigate. By the time an endoscopy was performed, everything was observed as clear with the exception of a likely-incidental mild eosinophilic oesophagitis, likely due to a 2cm sliding hiatus hernia causing reflux, impacting the lower oesophagus. After transiently being on-and-off the topical steroids, gastroenteritis symptoms repeatedly appeared shortly after every reintroduction of hydrocortisone sodium phosphate.
It was concluded in agreement with the gastroenterologist that the topical eye drop steroids were causing the gastritis, regardless of any previous information relating to oral high-dose patients, which typically suggest that gastritis is extremely unlikely with a low topical dose.
Due to this episode, it is clear to me that the gastritis risks of steroids are understated, though clearly not a reason to prevent their use entirely. More information is required on what factors contribute to topical eye-drop steroids causing gastritis, especially the incidence rate in users of topical ‘soft’ steroids such as hydrocortisone sodium phosphate.
Curtis Holt
